Here comes Hank. Too late, he’s spotted you, and now you’re in for another story—or rather, a litany of unnecessary details. “I said this, and she said that, and then I said, ‘Really!’” Hank never edits himself; he simply tells you E-V-E-R-Y-T-H-I-N-G until you’re screaming inwardly, “Get to the point!”
While editing manuscripts, I periodically encounter a “Hank” author. Every tidbit of information is important and, in his view, absolutely necessary. Along with his manuscript, which includes the maximum-allowed 5 tables and/or figures, he provides a Supplement that comprises 3 eMethods sections, an eResults, 14 eTables, and 9 eFigures. Data, data, and more data, until the Supplement resembles a closet stuffed by an 8-year-old who was told to clean her room. Everything. It’s all in there.
Consider the busy physician-reader. After perusing the array of freshly published articles in the journal website’s New Online section, she may click on Hank’s title and see that long list of supplemental material populating the scholar’s margin. However transparent the author endeavored to be by providing so much information, she doesn’t have time to read it all now; she needs summaries.
AMA style advocates that “tables and figures demonstrate relationships among data and other types of information” and that “a figure should be used if the relationships are complex….Like a paragraph, each…figure should be cohesive and focused.”
With that reader in mind, the manuscript editor reformats the author’s originally supplied figures to journal style and hones each one to present the material clearly. No chartjunk, no extraneous elements, no distracting line treatments.
Flow diagrams show the numerical progression of patients through the study: the number screened for inclusion, the number excluded for these reasons, the number enrolled, and the number at each stage, with those excluded or lost to follow-up at each stage also accounted for. The last box shows how many patients made it to the end of the study or were included in the primary analysis. From top to bottom, the progression of numbers makes perfect arithmetic sense.
Figures of multiple clinical, radiologic, or histologic images are labeled to guide the reader: before surgery, 6 months after surgery, 2 years later; magnetic resonance images of brains from patients 1 and 4; or specimens from a healthy individual and a patient with disease preceding another from the patient 1 year after treatment.
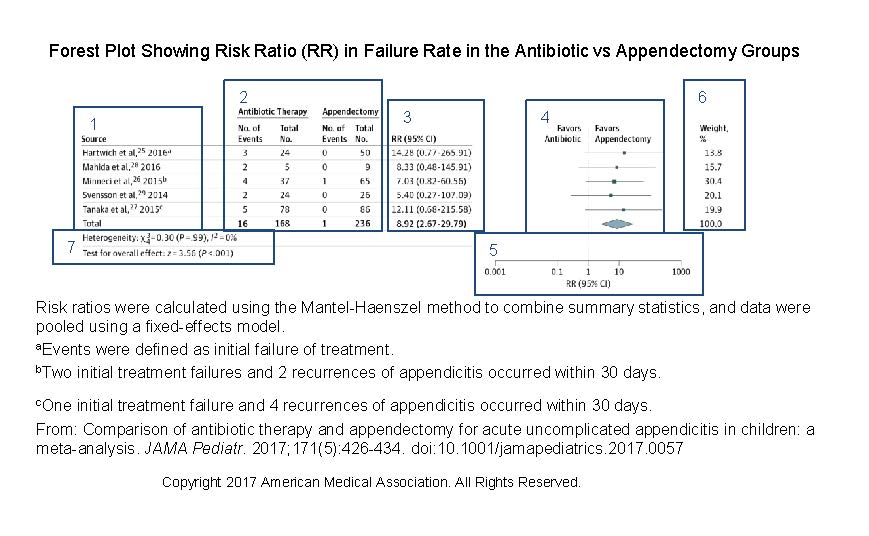
Graphs are appropriate to the data presented: bars for frequencies, data markers and error bars for summary data, forest plots for meta-analyses. All axes and ticks are clearly labeled, curves are identified by direct labeling or by the inclusion of concise figure keys, and bars and data markers are a solid color for the patients who received treatment and without color for those who received placebo. The numbers of patients at risk at each time point lend additional meaning to Kaplan-Meier survival curves. Forest plots include numerical data in addition to the illustrated plot points, with labels on either side of the graph’s vertical line at 1.0 to indicate whether each data marker’s location favored treatment or no treatment.
Back to our reader. Time is short, so she starts with the abstract. Words are read quickly, their meaning filtered through her years of accumulated knowledge and absorbed. She takes in the tables next. Row upon row of data; numbers represent baseline characteristics, laboratory results, and statistical analysis. Again, the numbers are filtered for meaning and digested for information that can help the reader treat her own patients. She studies the figures, and their meaning is immediately apparent: the bar for affected patients from one age group is taller, a survival curve is higher and longer for patients who received the lower dosage, the difference between 2 clinical images before and after treatment is obvious. No filter needed. Instantly clear. Results from years of the author’s research are visually summarized, seen by the reader, grasped, and understood.
The Supplement stands ready for closer investigation, but first the point must not be obscured. State it—illustrate it—clearly.—Connie Manno, ELS