The recent outbreak of monkeypox disease (caused by the monkeypox virus), like COVID-19 and other pathogens before it, raised concern about disease names, particularly those that could negatively affect particular nations, populations, or animals.
The naming of diseases (and in this case, renaming) falls to the World Health Organization (WHO). After reports from individuals and countries raised concerns about the term “monkeypox” being racist or stigmatizing, the WHO met with concerned parties and invited public comment to rename the disease.1
The result is “mpox.”
The AMA Manual of Style will add the term “mpox” to the viruses section in the Nomenclature chapter (14.14) as well as information about the renamed clade I and clade II (formerly Central African and West African, respectively).2
We recommend dual reporting, such as mpox (monkeypox), at first mention to ease adoption of the new terminology. Other organizations, such as the Centers for Disease Control and Prevention3 and AP Stylebook,4 have also announced their adoption of the updated terminology.
The monkeypox virus name has not yet been changed. The International Committee on the Taxonomy of Viruses is responsible for that terminology,1 and when new nomenclature is announced we will update the Manual accordingly.
The AMA Manual of Style will soon offer guidance on inclusive language when referring to people who are pregnant or people with the capacity for pregnancy.
This wording has more general use and can include individuals who were assigned female at birth, transgender men, nonbinary individuals, gender-nonconforming individuals, and gender-fluid individuals–basically anyone who is physically able to become pregnant.
This language should be used when study investigators have not explicitly asked participants to self-identify their gender. In studies in which participants have all identified as women, it is appropriate to use terms like pregnant women.
However, if study participants have not completley self-reported their gender as women, terms such as pregnant participants, pregnant individuals, and pregnant patients are more accurate. In these cases, birthing parent rather than mother is a more accurate term and should be used for the same reasons.
There’s a scene in the film Pirates of the Caribbean: The Curse of the Black Pearl in which the heroine, Elizabeth, is taken captive by the infamous Captain Barbosa aboard his ship. In an attempt to negotiate her release, she invokes the Pirates Code, a set of rules to which she knows Barbosa is beholden. Barbosa initially appears to comply, then abruptly reneges. When Elizabeth protests his disregard for the Code, Barbosa defends his decision with a snide retort:
“The Code is more what you’d call guidelines than actual rules.”
His deviousness aside, the Captain has a point. As humans, we have an innate tendency to create rules with the intent of establishing order and certainty, yet those rules are occasionally subject to exceptions, inapplicability, and multiple interpretations. Try as we might, it’s virtually impossible to anticipate every possible scenario and account for it, which means there will be times when the rules we make for ourselves simply do not apply—and editorial style rules are no exception.
The question is: does style always supersede substance?
The AMA Manual of Style is a renowned and authoritative reference manual, and for good reason. It’s a meticulously crafted, oft-updated repository of linguistic and stylistic information steeped in authentic medical language and policy, and the guidance within its pages is critical to physicians, authors, and editors alike.
In that sense, the argument could be made that when it comes to the AMA Manual, style is substance. However, as editors, we at times find ourselves in scenarios in which adhering to a particular style point is akin to the proverbial placement of a square peg in a round hole. The gadget doesn’t quite fit into the device, and the results can be ugly. It’s those circumstances in which the absence of a peg may be preferable to the sight of a horribly splintered one.
What’s more, rules are almost always subject to change, and depending on the impetus behind an amendment, it can take the purveyors of a style manual weeks, months, even years to discuss and formulate a responsible and sustainable update before disseminating it to the manual’s users.
Take the topic of race and ethnicity language (Chapter 11.12.3), which continues to evolve at an unprecedentedly rapid pace—enough so that the requisite section in the AMA Manual was updated less than a year after the release of the 11th edition.1 Language and terms that may have been deemed acceptable just months previously may shift suddenly, and the intuitive and attentive editor may need to set aside current style guidelines to align with cultural and/or societal trends.
That said, style deviations should be made only after careful consideration of the potential ramifications, especially those involving reader perception. In other words: if you’re going to deviate from style, you’d better have a really good explanation ready.
Authors are often quick to point out style infractions in previously published material, either to defend their own infringements or to object to style-adherent edits (“If this author got to do it, why can’t I?”), and trivial or inexplicable noncompliance can undermine the authority of your style manual as well as your publication. If you can’t justify a style detour that goes beyond “I just thought it sounded better that way,” you probably shouldn’t take it.
Fictional though he may be, I expect that Captain Barbosa fully honors the Pirates Code—he is a pirate, after all. Yet even he knows to adapt the rules when necessary to achieve his goals. This is not to suggest that editors should swashbuckle their way through a manuscript, playing fast and loose with the style rules they’ve sworn to uphold. Those rules are there for a reason, and they wouldn’t exist if they didn’t almost always apply.
However, absolutism is fraught with its own perils, and the astute editor must be mindful of those rare situations in which a rule may need to be bent—or perhaps broken—for the greater good. And although there’s no single, comprehensive answer to the question of whether and when to sacrifice style for substance, if preserving the integrity of a publication is given precedence, the answers will at least be easier to identify.
Reference
Frey T, Young RK. Race and ethnicity. In: Christiansen SL, Iverson C, Flanagin A, et al, eds. AMA Manual of Style: a Guide for Authors and Editors. 11th ed. Oxford University Press; 2020:545-547.
The islands of Hawaiʻi and its people have a culture rich in history, traditions, and the Native Hawaiian language.
Sadly, use of the Native Hawaiian language began to decline in 1896, when it was banned from schools just 3 years after the Hawaiian monarchy was overthrown.1 Without being taught in schools, the Native Hawaiian language became dangerously close to being completely forgotten. By the early 1980s, fewer than 50 children spoke the language.2
A resurgence in cultural pride and identity in the 1970s led to the resurgence of many Native Hawaiian cultural traditions, including the language.
With this in mind, the AMA Manual of Style strives to be accurate, fair, and respectful in reflecting the identities of individuals and groups. The Manual is adding 2 diacritical marks used in Native Hawaiian to the Accent Marks (Diacritics) section (chapter 12.2).
The okina (ʻ) is a glottal stop and the kahakō is a macron (ā) that lengthens and adds stress to the marked vowel.
The marks are used throughout the language, including in many of the names of the main Hawaiian islands (eg, Hawaiʻi, Kahoʻolawe, Kauaʻi, Lānaʻi, Molokaʻi, Niʻihau, and Oʻahu).
Note that Hawaiʻi has 2 official languages according to the state constitution: English and Hawaiian.3 “Hawaiian” is considered an English word, so it doesn’t take the okina.
I have used many adjectives to describe myself, but I’ve never referred to myself as other. When teachers called my name during morning attendance, I responded by saying “Here.” I never said, “Invisible.”
In medical literature, the failure to fairly and respectfully recognize and include individuals of all races and ethnicities can severely adversely affect patients’ lives and the quality of care they receive. It can misinform clinicians. It can compromise the credibility of a journal.
This means that race and ethnicity data should be reported in a way that encourages fairness, equity, consistency, and clarity in medical and science journals.1
Changing the b in Black and the w in White to uppercase lettering when describing race is not about mere political correctness—these changes are part of a conscientious movement toward equitable delivery of health care services to all people.
The objective of this post is to emphasize that updated guidance about the reporting of race and ethnicity is important, not because the AMA Manual of Style says so, but because inattentiveness to these changes can contribute to unconscious bias and ultimately affect how patients are treated or unintentionally mistreated.
Bias, when unintentional, is not mitigated—it remains bias all the same. Unintentional bias can occur simply because the writer or editor is removed from the patient’s life experience. When the writer or editor is unaware, they may not recognize how insensitive wording can affect the reader.
Example: “Adherence to the prescribed medication was higher among White patients than among Blacks.”
Consequence: Does this mean that if you are White you are a patient but if you are Black you are nothing? What is a Black?
When a person is called a Black instead of a Black patient or a patient who is Black, the wording detracts from that person’s humanity.
Likewise, use of lowercase lettering for Black and White, as well as referring to people as minorities instead of as members of a racial or ethnic minority group, also diminishes their humanity. Stating race or ethnicity in noun form can be interpreted pejoratively and is akin to labeling patients by their disease (eg, the blind, schizophrenics, epileptics) instead of putting the individual first (eg, a person with schizophrenia).2 Other things that can be interpreted pejoratively and should be avoided are using the term mixed race, which can carry negative connotations, instead of multiracial or multiethnic, merging race and ethnicity with a virgule (ie, race/ethnicity) rather than recognizing the numerous subcategories within race and ethnicity with the term race and ethnicity, and using abbreviations for racial and ethnic terms. Although the writer or manuscript editor may not have intended to negatively portray a group of people, the potential effect on readers remains unchanged.
To potential authors, the absence of a single word can indicate that a journal is insensitive to the health care needs of a population of patients.
To clinicians with the same racial or ethnic background as the one negatively represented, this can promote the inference that the journal has no diversity on its editorial board or staff.
To a practicing physician, this language can translate to offensive or insensitive communication when speaking with a patient or a patient’s family member.
To a patient, this wording can indicate that the medical community views individuals from their racial or ethnic group as nonpersons—unseen, unconsidered, and uncared for.
For all of these individuals, this can deepen a sense of mistrust.
Language that excludes a racial or ethnic group can subtly influence a medical trainee to “unsee” the humanity in people who are from a different background. If their research and educational sources are written or edited without intercultural competence, the medical trainee may unintentionally miscommunicate or make incorrect assumptions about patients from other backgrounds. This breach can interfere with a clinician’s understanding of the patient and, in response, impede the patient’s trust in the clinician.
Among some patients from communities that have been medically underserved or ignored, information about medical mistreatment can transcend generations. Past miscommunication can lead to mistrust, which can then lead to fear.
A family may never forget that Grandma never came home from the hospital and that no clinician took the time to explain why. Although this family was made to feel invisible because of miscommunication, it is quite possible that the clinician intended no disrespect and had no knowledge of how the family was affected. A patient with a historic burden of oppression can potentially interpret disrespectful communication as an initial step down the road to medical abuse.
My godfather once expressed such fear. He was Black, the clinicians were White, and he had grown up in Mississippi during the 1940s. Although I asked, he refused to ever repeat details of what was said by these physicians many years ago. But decades later, when I was a teenager and a novice driver, my godmother phoned and urgently asked that I come to their home immediately to rush him to our local VA hospital.
On my arrival, she exclaimed, “I think he had a heart attack while gardening in the back yard!” I said, “I’ll call 911. The ambulance will get him there faster.” Then, she stopped me. She pleaded that I drive him there myself. As I rushed to his aid, she continued by telling me that he would die of fear if an ambulance came to their home. She told me that I must speak for him when we arrived, remain by his side, and do everything in my power to keep him calm.
He cried like a baby during the entire ride. He was afraid. He was humiliated about expressing fear in my presence. I did not know what to say. I just kept driving. My heart was broken.
This brief story is an example of deep-seated fear that some Black people experience in a health care setting, a fear that can only begin to be abated with a conscientious effort to ensure that language humanizes Black patients and patients from all racial and ethnic backgrounds.
How does one address suboptimal reporting on race and ethnicity?
First, follow the guidelines.
Second, write and edit with a raised antenna. Look for what is unsaid in addition to what is written on the page.
Try to interpret as if you are a person from a racial or ethnic group unlike your own. Think about how you would you feel as the subject or nonsubject of the article.
Consider how wording can be misinterpreted.
Consider how inattentiveness to detail can affect the health, safety, or life of someone who is misrepresented.
Edit responsibly, but without fear of respectfully questioning the author.
Remember: no one is invisible, and no one is other.
“Not everything that is faced can be changed, but nothing can be changed unless it is faced.”3
James Baldwin
References
Flanagin A, Frey T, Christiansen SL; AMA Manual of Style Committee. Updated guidance on the reporting of race and ethnicity in medical science journals. JAMA. 2021;326(7):621-627. doi:10.1001/jama.2021.13304
Christiansen SL, Iverson C, Flanagin A, et al, eds. Correct and preferred usage. In: AMA Manual of Style: a Guide for Authors and Editors. 11th ed. Oxford University Press; 2020:547-548.
H Ford, they/them/theirs, Manuscript Editor, JAMA Network
There is a particular type of online pedant whose view of the English language has the effect of invalidating strangers’ sexual and gender identities. Much physical and digital ink has been spilled discussing the validity of the singular “they” when referring to a single gender-unknown subject of discussion and as an intentional personal pronoun.
I will not relitigate this issue here, but it should suffice that the AMA Manual of Style (sections 11.12.2 and 7.2.3.2, specifically) concurs with the Chicago Manual of Style, the AP Stylebook, and historical use (eg, Shakespeare and Emily Dickinson) in permitting the singular they.
Now with that said, let’s talk about respecting our queer friends, family, colleagues, and authors by using the honorific Mx! According to Merriam-Webster, the first use of the gender-neutral honorific Mx was in the 1970s, but its widespread use has only gained momentum within the past 5 to 10 years.
It can be helpful to compare Mx with Ms, another relatively recently developed honorific. Although the very first publication of the honorific Ms was in a 1901 article and was likely more focused on expediency of the address than the linguistic and sociopolitical ramifications of defining a woman by her social status, most people’s understanding of Ms is rooted in Gloria Steinem’s eponymous magazine (https://www.nytimes.com/2009/10/25/magazine/25FOB-onlanguage-t.html).
Mx is an honorific that affords the same respect to nonbinary and gender-nonconforming people that has traditionally been given to gender-conforming individuals who do not hold advanced degrees. As awareness grows of the existence of gender identities outside the male/female binary, more people every day feel comfortable publicly identifying as nonbinary, genderqueer, and agender.
The widespread use of Mx signals acknowledgment of and respect toward these individuals. Yet there is a broader application of the honorific Mx that we haven’t fully considered, one that is as practical as it is gender inclusive. Just as the title Ms allowed us to ask why a woman’s marital status affected how she was addressed, Mx should allow us to ask why a person’s gender should matter to any respectful form of address.
For these reasons, JAMA Network now offers Mx as a salutation for submissions to all of its journals!
As editors and writers, we occupy a unique position in the process of the legitimization of nascent linguistic terms. Let’s use that power for good!
Eman Hassaballa Aly, Social Media Manager; Reuben Rios, Social Media Coordinator; Deanna Bellandi, MPH, Manager, Media Relations (JAMA Network)
“All we want are the facts.”
Sgt Joe Friday, Dragnet
Social media is an important tool for promoting content published in JAMA and the JAMA Network family of journals to the research community, physicians and other health professionals, and lay audiences. Doing that means following a set of guidelines meant to ensure accurate and responsible social media posts.
JAMA Network Social Media Guidelines
Content published in social media sites is subject to the same norms, standards, and regulations as is all other published content.1
Be respectful.2
Use proper grammar, spelling, and capitalization.3
Abbreviations may be used provided they can be easily understood in context.
Avoid texting jargon, such as “U” for “you” or “L8” for “late.”3
Do not use sarcasm, irony, satire, or absurdities.4
Reflect diversity.4
Use language that is nondiscriminatory.5
Do not include negative comments directed at any person, group, or institution.
Do not use offensive content (including, but not limited to, racist, sexist, ageist, anti-LGBTQ, and antireligious.)6
Do not include sexually suggestive images or video (eg, genitalia, breasts, buttocks) or those that portray sexual assault/abuse.
Do not use language, images, or other content that reinforces stereotypes.5
Use individuals’ preferred pronouns when known; inclusive pronouns (they/them) are acceptable.4,5
When reporting the results of a study or describing a specific journal article, replace personal pronouns (I and we found) with reference to the study or the article type (eg, Viewpoint, Review).
When mentioning people/Twitter handles, do not editorialize or designate appellations (eg, do not say, “The great [@Twitter handle] discusses…”).
Do not use profanity or vulgarity.2,6
Do not include emojis based on gender or race.4
Do not include identifiable patient content without permission.1
Do not share confidential information.7
Do not share information that is embargoed or before publication date and time.
Do not include quotes, images, photos, or video from other social networking sites or third-party publications without permission and attribution to the source.8
Do not share others’ social media posts that do not follow these guidelines.
Correct posts with errors transparently and as soon as possible. For example, add a new post clarifying the correction, and include the word “correction.”
Posts that do not follow these guidelines may be removed.
Tweet Formatting
The basic format of a tweet consists of text, links, and hashtags handles with optional attached video and images (up to 4 images per tweet).
Length: the maximum length for JAMA Network tweets is 257 characters. Twitter limits to 280 characters, but because JAMA Network always includes a link, 23 characters are reserved for the link.
Hashtags should be limited to 3 per tweet.
Twitter handles should be included if there is room. Handles should be limited to authors and institutions directly related to the content of the tweet.
Example: Tweet text (including relevant @mentions and #hashtags), Link, Other @mentions (if not directly mentioned in the tweet), Other hashtags (if any, and if space permits).
Today is the start of Peer Review Week, an annual global event celebrating the essential role that peer review plays in maintaining scientific quality. This year’s focus is on trust in peer review, and this post addresses the evolving transformation of the peer review in scientific publication.
Peer review continues to develop, albeit slowly, in terms of models and methods, with increasing calls for openness and transparency. There are 3 common forms of peer review:
Double-blind review: Authors’ and reviewers’ identities are hidden from each other in an attempt to minimize bias.
Single-blind review: Authors identities are revealed to all, but reviewer identities are not revealed to authors (also known as anonymous review)
Open review: Author and reviewers are identified are revealed and various levels of the process and outputs may or may not be made public
Types of open review, with increasing levels of openness, include the following:
Level 1: Reviewer and author identities are revealed to each other during the peer review process
Level 2: Indication of editor and/or reviewer names on the article
Level 3: Posting of peer review comments with the article, signed or anonymous
Level 4: Publication of peer review comments (signed or anonymous) with authors’ and editors’ responses, decision letters, and submitted and revised manuscripts
Level 5: Publication of the submitted manuscript after a quality check and inviting public discussion from the community
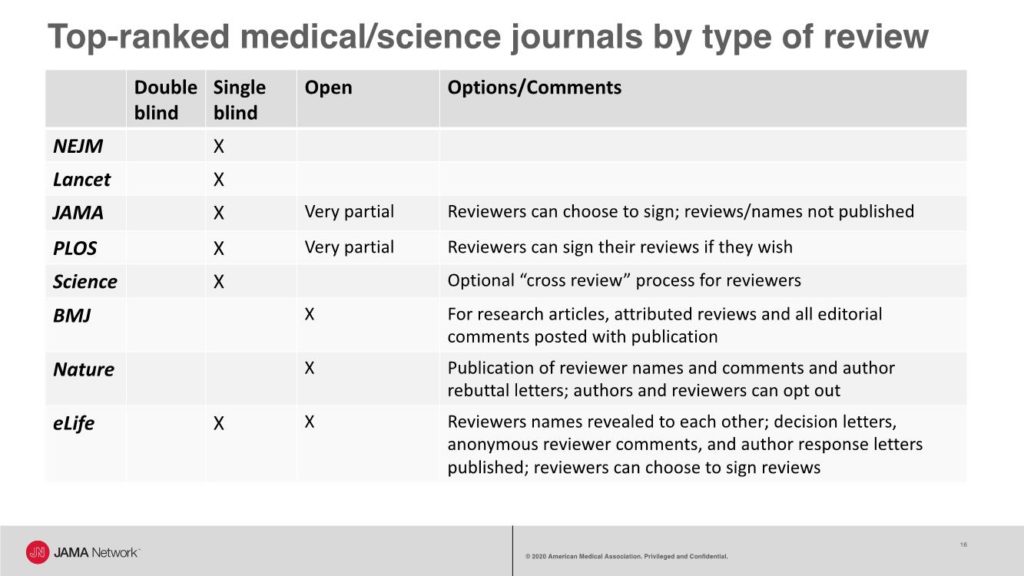
A recent look at the types of peer review used by some top-ranked general medical and science journals shows that most journals use single-blind review, with some allowing reviewers to choose to sign their reviews. For example, JAMA has a single-blind review process and offers reviewers the option to sign their reviews that are shared with authors, and copies of reviews are shared with other reviewers.
JAMA also has an editorial collaborative process, called editorial review before revision, during which senior editors, a manuscript editor, and an editor with expertise in data display collaborate to provide guidance to the authors on all that is needed during revision to reach a favorable final decision.
However, these processes are not public. A short video that explains an inside view of the editorial and peer review process at JAMA is available.
JAMA Network
The BMJ has a fully open review process with the following published with all research articles: all versions of the manuscript, the report from the manuscript committee meeting, reviewers’ signed comments, and authors’ responses to all comments from editors and reviewers. Nature publishes reviewer names and comments and author rebuttal letters; however, authors and reviewers can opt out of the open review process. And eLife has a mixed model with reviewers’ names revealed to each other during the review process; decision letters, anonymous reviewer comments, and author response letters published with the article; and an option for reviewers to sign their reviews.
One of the earliest demonstrations of open and collaborative peer review was launched in 2001 by Copernicus Publications, an open-access publisher of scientific journals. These journals use a 2-stage process:
“In the first stage, manuscripts that pass a streamlined access review are immediately posted as preprint in the respective discussion forum. They then undergo an interactive public discussion, during which the referees’ comments (anonymous or attributed), additional community comments by other members of the scientific community (attributed), and the authors’ replies are posted. In the second stage, the peer-review process is completed and, if accepted, the final revised papers are published in the journal.”1
Many studies have compared the quality of single-blind, double-blind, and open review. Early randomized trials2,3 found no differences in the quality of double-blind, single-blind, or open review. But some studies have found differences, such has higher quality for blinded review,4 higher quality for signed reviews,5 and higher quality for open review.6 And some studies7,8 have identified biases that may be better managed with double-blind review (eg, bias toward gender, geography, institutions, and celebrity authors). However, no study has yet compared the quality of published articles that have undergone these different types of peer review.
“The predominant system of editorial review, where the names of the reviewers are unknown to the authors, is a perfect example of privilege and power (that of the reviewer over the fate of the author’s manuscript) being dislocated from accountability….to the fellow scientist who wrote the manuscript. For that reason alone, we must change our practices. ….The arguments for open peer review are both ethical and practical, and they are overwhelming.”9
There have also been numerous studies demonstrating the feasibility of each type of peer review. However, some studies have found that double-blind review is not always successful and have reported rates of failure to ensure blinding ranging from 10% to 40%. Other studies have found that reviewers who are asked to sign their reviews may be more courteous or positive in their recommendation, may take longer to complete their reviews, and may be more likely to decline invitations to review.
Support for open review, with options, continues to evolve. In a 2016 OpenAire survey of 3062 academic editors, publishers, and authors,10 60% indicated that open peer review (“including making reviewer and author identities open, publishing review reports and enabling greater participation in the peer review process”) should be common in scholarly practice, but they had some concerns. For example, 74% responded that reviewers should be able to choose to participate in open review, and 67% reported being less likely to review if open review was required.
The Nature journals have been experimenting with various models of peer review, and in 2016, Nature Communications announced that about 60% of its authors agreed to have their reviews published.11 In 2019 and 2020, Nature journals began offering “transparent peer review” with options for authors and reviewers to opt out.12
Elsevier conducted a pilot of open review from 2014 to 2017 in 5 journals, with reviews published.13 During this pilot, younger and nonacademic scholars were more willing to review and provided more positive and objective recommendations. There was no change in reviewer willingness to review, their recommendations, or turn-around times. But, only 8% of reviewers agreed to reveal their identities with the published reviews.
Thus, the key to successful transformation to open peer review and maintaining trust in the process may be offering options to authors and reviewers. Whichever model is used, journals should clearly and publicly describe their processes (eg, in Instructions for Authors) and continue to evaluate and test ways to improve the peer review process for authors, reviewers, and editors.–Annette Flanagin, Executive Managing Editor and Vice President, Editorial Operations, for JAMA and the JAMA Network, and Executive Director of the International Congress on Peer Review and Scientific Publication
*Note: Portions of this post have been presented at several meetings.
Justice AC, Cho MK, Winker MA, Berlin JA, Rennie D; PEER Investigators. Does masking author identity improve peer review quality? a randomized controlled trial. JAMA. 1998;280(3):240–242. doi:10.1001/jama.280.3.240 https://jamanetwork.com/journals/jama/fullarticle/187758
van Rooyen S, Godlee F, Evans S, Smith R, Black N. Effect of blinding and unmasking on the quality of peer review: a randomized trial. JAMA. 1998;280(3):234–237. doi:10.1001/jama.280.3.234 https://jamanetwork.com/journals/jama/fullarticle/187750
McNutt RA, Evans AT, Fletcher RH, Fletcher SW. The effects of blinding on the quality of peer review: a randomized trial. JAMA. 1990;263(10):1371–1376. doi:10.1001/jama.1990.03440100079012 https://jamanetwork.com/journals/jama/fullarticle/380957
Walsh E, Rooney M, Appleby L, Wilkinson G. Open peer review: a randomised controlled trial. Br J Psychiatry. 2000;176(1):47-51. doi:10.1192/bjp.176.1.47
Bruce R, Chauvin A, Trinquart L, et al. Impact of interventions to improve the quality of peer review of biomedical journals: a systematic review and meta-analysis. BMC Medicine. 2016;14(85). https://doi.org/10.1186/s12916-016-0631-5
Lerback J, Hanson B. Journals invite too few women to referee. Nature. 2017;541(7638):455–457. doi:10.1038/541455a
McGillivray B, De Ranieri E. Uptake and outcome of manuscripts in Nature journals by review model and author characteristics. Res Integr Peer Rev. 2018; 3(5). https://doi.org/10.1186/s41073-018-0049-z
Rennie D. Freedom and responsibility in medical publication: setting the balance right. JAMA. 1998;280(3):300–302. doi:10.1001/jama.280.3.300
Ross-Hellauer T, Deppe A, Schmidt B. Survey on open peer review: attitudes and experience amongst editors, authors and reviewers. PLOS One. 2017;12(12): e0189311. https://doi.org/10.1371/journal.pone.0189311
Bravo G, Grimaldo F, López-Iñesta E, et al. The effect of publishing peer review reports on referee behavior in five scholarly journals. Nat Commun. Published online Junary 18, 2019. https://doi.org/10.1038/s41467-018-08250-2
Since I’ve been a manuscript editor, JAMA Network journals have published a few articles about health care for transgender patients. I’ve had the good luck to edit a few—they are always interesting—but this week, I realized that there is a grammatical issue in editing these articles that I have never heard fully addressed.
The issue is not what pronouns to use for transgender individuals—that question is well-known. Because the English language uses gendered pronouns, people who change their gender expression or whose gender isn’t accurately defined by labels are faced with several choices: should they go by she, he, a singular they, or a neologism, such as xe?
The news media has addressed this, including The New York Times articles in 2016 and 2017, with another written by transgender English professor Jennifer Finney Boylan in 2018. These articles often make the same points: that people can get confused by this transformation of language, but that people who want to use pronouns that reflect a gender different from their assigned sex should have their wishes respected. This squares with the approach used in JAMA Network journals.
But it also raises a question rarely addressed: what about verb conjugation? In the present tense, English applies a letter s to the third-person singular (he, she, or it runs) but not to the first-person singular, first-person plural, second-person singular, and third-person plural (I, we, you, and they run). So, if an article uses a singular they, should it be conjugated like the third-person plural (run) or like the third-person singular (runs)?
While editing, I have realized that the default method of using the singular they along with someone’s name (or a descriptor, such as the patient) involves flip-flopping between singular and plural verb conjugations (eg, “The patient is receiving gender-affirming treatment, and they are pleased with the outcome thus far”). A consistent use of the singular they would seem to require using third-person singular conjugations throughout (“The patient is receiving treatment…. They is pleased…”) or plural conjugations throughout (“The patient are receiving treatment…. They are pleased….”). Is either approach correct?
The public discourse on pronouns has not provided much insight. It has prompted the argument that we all use forms of singular they-series pronouns in casual language, in sentences such as “If someone wants gender-affirming treatment, that is their choice” or “Give them an injection.”
But that is distinct from the current issue. In these usages, the pronoun is usually objective (them) or possessive (their or theirs), and the verb is conjugated in the third-person singular alongside another subject. (In the example sentences, these are “someone” and “that,” and in the command, an unspoken “you.”) When the singular they is placed immediately before the verb, the question of conjugation instantly reappears.
Weighing “they run” vs “they runs,” I looked for guidance in the AMA Manual of Style. It offered a few relevant thoughts: “In an effort to avoid both sex-specific pronouns and awkward sentence structure, some writers use plural pronouns with singular indefinite antecedents… Editors of JAMA and the Archives Journals prefer that agreement in number be maintained in formal scientific writing.”
But that seemed short of clear instructions. Still uncertain if constructions like “they is pleased” would please anyone, I reached out to Jennifer Finney Boylan, the New York Times contributor whose article on pronouns was published in 2018.
A quick email to her university address got an equally quick response. “I’m not certain about this,” she wrote. “I want to endorse ‘they is’ because the non-specific pronoun is still referring to a singular individual. On the other hand, ‘they are’ sounds better to my old, English professor ears.”
That seemed similar to how our society is handling the matter. On her authority, I decided to stick with conjugations that shift from singular to plural and let the matter rest until a thoughtful body of grammarians, popular opinion, and perhaps the next edition of the New York Times’article series on pronouns weigh in with a definitive answer to conjugating verbs after a singular they.—M. Sophia Newman
Sometimes before I go to bed, I like to check in on one of my favorite YouTubers, Dr Pimple Popper (the nom de internet of dermatologist Sandra Lee), who posts videos of dermatologic procedures and skin care treatments. I particularly enjoy watching videos of dilated pore extractions, and I don’t mind watching lipoma extractions either (although I do sometimes fast-forward through the excisions). I know these types of videos can get viewers’ stomachs churning a bit, but I think it’s no worse than various photographs in medical journals I have worked at over the years. And because of my occupation, I do wonder about patient privacy and anonymity.
Patients featured on this YouTube channel may have a cyst near their eye or ask for blackheads to be removed from their cheek, and their faces are clearly visible. In many videos, Dr Lee chats with her patients, and although she sometimes edits out personal details, some of it stays. Dr Lee says that patients do sign consent forms before videos are published.
Similarly, when manuscript editors of medical journals encounter photographs of patients, we must review whether the photograph might intrude on patient privacy. Authors must obtain written permission from patients (or their legally authorized representatives) for any descriptions, photographs, or videos of patients or identifiable body parts and indicate that such consent was obtained in the Methods or Acknowledgment section. When I started in this field as an editorial assistant, I processed a manuscript that described a skin lesion on a patient’s back. In an accompanying photograph, the patient’s distinctive tattoo was visible, and I needed to ask the author to either obtain patient consent or have the photograph cropped because the patient (as well as anyone who knew he had that tattoo) would be able to identify himself. Results of imaging studies and photos of laboratory slides may also have identifying information that should be removed.
Protecting patient privacy also extends to
what is in the text of an article. When editing case descriptions, case
reports, and personal essays, nonessential identifying data (eg, sex, specific
ages, race/ethnicity, occupation) should generally be removed unless the author
has permission or the information is clinically or scientifically relevant and
important. Authors and editors should not falsify or fictionalize details; doing
so may introduce false or inaccurate data.