Timothy Gray, PhD, JAMA Network
If you’re eating candy, it’s “3 Musketeers.”
If you’re reading about the friends of d’Artagnan, it’s The Three Musketeers.
Given that JAMA Network publications are technical instead of literary (A Piece of My Mind and Poetry notwithstanding), we would fall on the candy side of the divide between using numerals and using words (whether candy is technical is a discussion for another day).
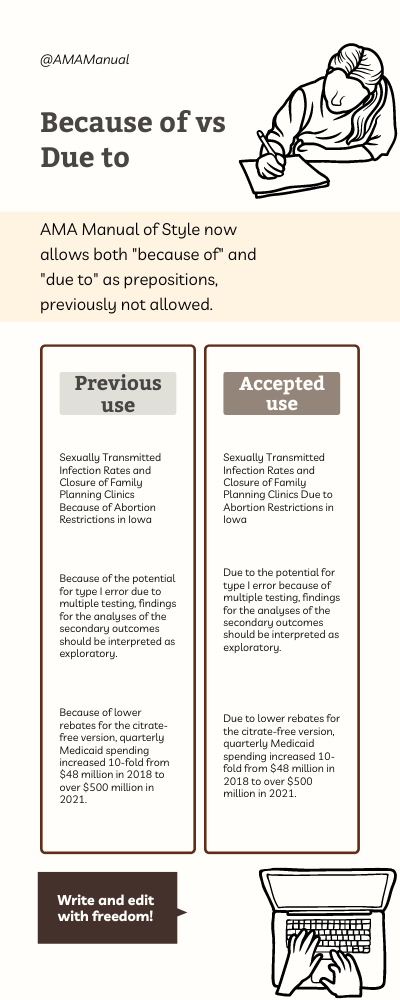
The online abstract to Chapter 18.0 in the AMA Manual of Style, Numbers and Percentages, raises “the difficult question of when to use numerals and when to use words, and how to combine the two.” Note the tidy example of spelling a number as a noun. This difficulty is a factor in what I see as numeral inflation in the form of encroaching “1” use.
One of the most obvious places for numeral use is in identifying study populations.
For example, take this hypothetical Delphi consensus group: 5 physicians, 4 nurse practitioners, 3 patient advocates, 2 patient caregivers, and 1 health system leader.
One of the most obvious places for spelled number use is in idiomatic phrasing or in parts of speech. Section 18.2.3, Accepted Usage, advises using words “in circumstances in which use of the numeral would place an unintended emphasis on precise quantity.” When a number appears in text, what is the cutoff point between intended and unintended emphasis?
The manual suggests that “common sense” plays a role in editorial judgment, but one person’s “common sense” is another person’s “thanks anyway.”
As examples of avoiding unintended emphasis on quantity, the style manual lists “one-time variables,” “in one recent case,” and “has become one of the dominant topics.” However, in current publications you will find encroaching “1” use in various “1-time” constructions, the phrase “in 1 recent analysis,” and the wording “has become 1 of the leading reasons.”
How about these uses of encroaching 1?
- “At least 1 moderate event.”
- “In 1 large health system.”
- “More than 1 time zone.”
Numeral use would seem to be justified by the idea that a moderate event, a large heath system, and a time zone are being counted.
Section 18.2.2 advises that we should spell “one” used as a pronoun or a noun, and these 1s are part of a noun phrase as the object of the prepositions “at least,” “in,” and “more than.”
I am “all for one.” It can be a relief to have an automatic edit to make in the name of upholding style, but many of us are not “one for all”—even in cases sanctioned by Accepted Usage. Not every “one” that seems countable should be “1,” and I offer this observation not to get editors into the weeds (an occupational hazard) but rather to help them avoid reflexive editing.
December 9, 2024